
How to Diagnose the Sick Meridian in Dr. Tan's Balance Method: The One-Finger Rule, Meridian Geography & Common Mistakes
Four patients in twenty minutes. That's what a busy Balance Method clinic looks like. The practitioner doesn't sit down to take a history, doesn't check the tongue, doesn't feel the pulse. Instead, he asks each patient the same question: "Can you show me with one finger exactly where you feel the pain?"
The first patient has wrist and thumb pain. She points to the radial side of the wrist — that's Large Intestine and Lung territory. The practitioner asks: "Does it radiate to the thumb, or is it only where you show me?" It comes up into the knuckle. Now he has a precise diagnosis: Lung/Large Intestine channel, wrist level, six months duration. He walks to the opposite foot, palpates near Liver 4 at the ankle, finds a reactive point, needles it. The patient moves her wrist: "Pretty good. All gone."
The second patient has left shoulder pain. But "shoulder pain" isn't a diagnosis. Where on the shoulder? The patient describes constant tightness, not movement-related, from too much computer work. The practitioner identifies the pain at the shoulder joint where it traverses the Large Intestine and San Jiao channels. Not Lung or Small Intestine. He needles Kidney 3 area on the opposite ankle. The pain area shrinks from a broad zone to a small spot. He adds one extra needle — and the remaining tension resolves.
Two patients, two completely different diagnoses, both called "pain in the upper limb." The difference? Precision in Step 1. The practitioner differentiated the exact meridian by asking the patient to show exactly where — and that one question determined the entire treatment.
Meridian Diagnosis, Not TCM Pattern Diagnosis
This is the most important shift for practitioners coming from a TCM background. In the Balance Method, diagnosis means identifying the sick meridian by location. You don't need to determine whether the patient has Liver Qi stagnation or Kidney Yang deficiency. You need to determine which meridian runs through the area where the problem expresses.
After treating four patients, you might ask me: 'Did you look at the tongue?' No. 'Did you take the pulse?' No. The patient's body gave me enough information through location alone. As taught in Balance Method training: Zang-Fu differentiation was developed primarily for herbal prescribing. It's not wrong — it's simply designed for a different purpose. The classical acupuncture approach, long before Zang-Fu theory existed, diagnosed by meridians. Dr. Tan returned to that original, location-based method.
Acupuncture vs TCM Diagnosis
| Aspect | Balance Method | TCM Zang-Fu |
|---|---|---|
| What you identify | Which meridian + where on it | Which organ pattern |
| Primary tool | Patient points with one finger | Tongue, pulse, questioning |
| Time needed | 30 seconds – 2 minutes | 10 – 30 minutes |
| Designed for | Acupuncture point selection | Herbal formula selection |
This doesn't mean you forget everything you learned in TCM school. It means you use the right diagnostic system for the right tool. Herbs need pattern differentiation. Needles need meridian location.
Meridian Geography: Where Each Channel Runs
To diagnose the sick meridian, you need one piece of knowledge that many practitioners surprisingly lack: exactly where each of the 12 meridians runs on the body. Not just the textbook point locations — the actual territory each channel covers.
The system is logical. Every limb has six meridians — three Yin on the medial (inner, white-skinned) side and three Yang on the lateral (outer, darker-skinned) side. The Chinese named them based on how much sun exposure each position receives.
The sun exposure logic
Stand with your arms by your sides, palms facing forward. The parts of your body that face the sun — the outer arms, the outer legs, the back — are Yang territory. The protected parts — inner arms, inner legs, the front of the trunk — are Yin territory. Now divide each side into three lines: front, middle, and back.
The front of the Yang side is still relatively protected — it's the most Yin part of Yang. That's Yang Ming. The back of the Yang side gets maximum sun exposure — that's Tai Yang. The side, between front and back, is Shao Yang. The same logic applies to the Yin side: front is Tai Yin, back is Shao Yin, and middle is Jue Yin.
Arm (6 Channels)
| Position | Yin (Medial) | Yang (Lateral) |
|---|---|---|
| Front | LU — Lung (Tai Yin) | LI — Large Intestine (Yang Ming) |
| Middle | PC — Pericardium (Jue Yin) | SJ — San Jiao (Shao Yang) |
| Back | HT — Heart (Shao Yin) | SI — Small Intestine (Tai Yang) |
Leg (6 Channels)
| Position | Yin (Medial) | Yang (Lateral) |
|---|---|---|
| Front | SP — Spleen (Tai Yin) | ST — Stomach (Yang Ming) |
| Middle | LIV — Liver (Jue Yin) | GB — Gallbladder (Shao Yang) |
| Back | KID — Kidney (Shao Yin) | UB — Urinary Bladder (Tai Yang) |
When a patient points to the lateral side of the knee, you see it's Yang territory, side position — that's Gallbladder. Medial knee, front position? Spleen. Posterior knee, medial? Kidney. The diagnosis happens in the time it takes to look at where their finger is pointing.
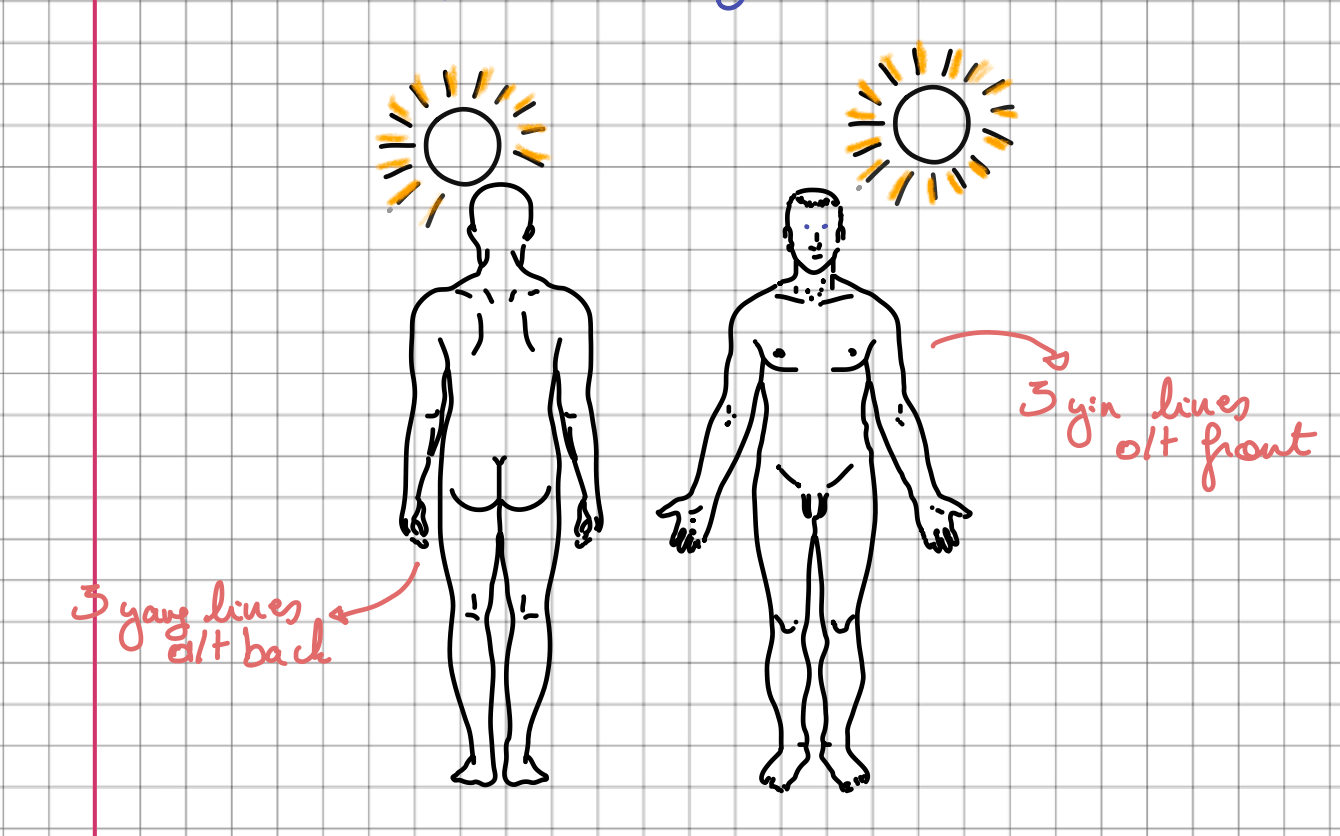
Image from the Balance Method Notebook by Laurence Meyfroodt
How to learn this fast
Practice on yourself. Place your arm palm-up on the table and trace the three Yin lines: Lung at the front (thumb side), Pericardium in the middle, Heart at the back (pinky side). Flip your arm and trace the three Yang lines: Large Intestine at the front, San Jiao in the middle, Small Intestine at the back. Do the same on the leg. Within a week of daily practice, you'll identify any meridian on any body part without thinking — the same way you read words without sounding out letters.
Three Things You Need to Know About the Problem
A good meridian diagnosis answers three simple questions:
1. Which meridian?
This is the core of Step 1. The patient points → you identify which meridian runs through that spot. Pain on the thumb side of the wrist? That's the Lung channel. Pain on the pinky side? Heart or Small Intestine. The meridian geography tables above give you this answer instantly.
2. Where on that meridian?
The same meridian runs from fingers to shoulder (or toes to hip). Where along its course is the problem? At the wrist? Halfway between wrist and elbow? Near the elbow? This matters because it determines where your projection will land on the treating meridian during Step 3.
The proportion matters too. If the problem sits one-quarter of the way from wrist to elbow, then your treating point should also be one-quarter of the way between the corresponding landmarks. Not just "somewhere on the forearm" — proportional to the landmarks.
3. How deep?
Is it at the skin surface, in the muscle, in the tendon, or down to the bone? This determines your needle depth. A superficial burning sensation needs a shallow needle. A patient who says "it feels deep, like it's in the bone" needs a needle that reaches the bone on the treating meridian. Bone for bone, tendon for tendon, muscle for muscle.
At the end of Step 1, you should be able to say something like: "Gallbladder channel, between knee and hip, about one-third up, muscle depth." That's a complete diagnosis — and everything you need to move to Step 2
The One-Finger Rule
The single most important clinical technique in Step 1: "Show me with one finger exactly where you feel the pain."
Why one finger? Because patients naturally generalize. "I have shoulder pain" could mean six different meridians. "I have back pain" could mean Urinary Bladder, Du Mai or Gallbladder — depending on whether it's midline, lateral, or between the spine and the scapula. When you force the patient to use one finger, they commit to a precise spot. That spot tells you the meridian.
If the pain covers an area rather than a point, ask them to trace it. The path they draw shows you which meridian (or meridians) are involved, and whether the problem is a point, a line, or an area. This directly impacts your needling strategy later: point for point, line for line, area for area.
Coverage principle
This distinction matters more than most beginners realize. If the patient shows you a single point of pain on the throat, you look for a single ashi point on the treating meridian. But if the patient traces a line from the upper throat (Stomach channel) down toward the chest, that line won't shrink to just a point when projected onto your treating arm — it will shrink proportionally to a shorter line. You then need to palpate along that projected line, not just at one point. As taught in training: when the problem is a line, you don't just palpate at Pc7 or Pc6 — you palpate from PC 7 to PC 6.5, looking for the most reactive zone.
Coverage Strategy
| Patient Presentation | → | Your Approach |
|---|---|---|
| A single point of pain | → | One ashi point on treating meridian |
| A line along the meridian | → | Proportional line, cover the projected zone |
| A broad area | → | Multiple needles to cover the area |
When Pain Falls Between Two Meridians
In real clinical practice, patients don't always point neatly onto one meridian. The pain often sits between two channels — for example, between Kidney and Urinary Bladder on the posterior medial leg, or between Liver and Spleen on the medial lower leg.
This is normal, and the Balance Method has a clear protocol for it.
Diagnosing the in-between
If the patient points to a spot that's about 50% between Kidney and Urinary Bladder, your diagnosis is: "in between Kid and UB." You then balance both. Kidney balances via its systems (Heart via System 1, San Jiao via System 2, etc.), and UB balances via its systems (Small Intestine via System 1, Lung via System 2, etc.).
Here's where it gets elegant. When you go to needle, you needle between the corresponding treating meridians too. If Kidney is balanced by Heart and Urinary Bladder is balanced by Small Intestine, you palpate between Heart and Small Intestine on the treating limb — in the same proportion. If the diagnosis was 50% between Kid and Ub, you palpate 50% between Ht and SI.
Using the matrix for in-between problems
Or — and this is the smarter approach for efficiency — you use the matrix to find one treating meridian that balances both sick meridians through different systems. A single meridian can balance more meridians with one set of needles instead of two. This is matrix analysis: the technique for managing complex, multi-meridian presentations with the fewest needles possible.
Multiple Locations, Multiple Meridians
Real patients rarely have one clean problem on one meridian. They come in with elbow pain on the San Jiao channel AND lower back pain on the Urinary Bladder channel AND a stiff neck on the Gallbladder channel. Three separate locations, three meridians.
The approach: list all sick meridians, map their balancing options through the matrix, and look for common treating meridians that cover multiple problems simultaneously. One meridian that appears as a balancing option for two or three of the sick meridians is your best choice — maximum coverage, minimum needles.
This is where the six systems become powerful: a single treating meridian can balance one sick meridian through System 1 and another through System 4, covering both with one set of needles.
Internal and Functional Conditions
What about patients without localized pain? Digestive discomfort, respiratory problems, insomnia, anxiety?
The principle remains: where does the problem express? About 80% of patients with internal conditions still have a local expression somewhere. A sinus problem expresses at the nose and eyes — that's Stomach and Large Intestine territory. Digestive pain expresses in the abdomen — Stomach, Spleen, Ren Mai. Chest tightness — Stomach, Kidney, Ren Mai.
Ask: "Where do you feel it the most?" Even vague symptoms like "tightness in the chest" give you a location, and a location gives you a meridian. Once you have the meridian, the Balance Method logic takes over — Global Balance for functional conditions, Local Balance for localized expressions.
For the small percentage of conditions with no local expression at all — pure insomnia with no physical discomfort, generalized fatigue without any specific pain — the diagnostic approach shifts to Global Balance patterns selected by constitution and Shen criteria, taught in advanced training programs.
Common Step 1 Mistakes
Step 1 is conceptually simple, which is precisely why beginners underestimate it. These are the errors that undermine everything that follows.
1. Accepting "shoulder pain" as a diagnosis
The most common mistake. The patient says "shoulder pain" and the practitioner jumps to treatment. But which part of the shoulder? Side is Large Intestine. on the back Small Intestine. top of the trapezius is Gallbladder. Each position demands a different treating meridian. The one-finger rule exists to prevent this exact error.
2. Diagnosing by Zang-Fu instead of location
You hear "lateral knee pain" and think "Gallbladder, Wood element, must be Liver Qi stagnation, I should add Liver 3 and LI 4." Stop. In the Balance Method, the only thing that matters for Step 1 is: the pain is on the Gallbladder channel at knee level. That's your diagnosis. Pattern differentiation is for herbs. Meridian location is for needles.
3. Skipping Step 1 to jump to Step 3
You've treated sciatica many times, you know which points work, so you go straight to needling without confirming the meridian. But this patient's sciatica might be on the Gallbladder channel while your go-to treatment targets Urinary Bladder. Never skip from Step 1 to Step 3. Always diagnose the meridian first, then choose the system, then find the point. The whole logic of Acupuncture 1-2-3 depends on this sequence.
4. Ignoring the depth
Two patients point to the same spot on the scapula. But one has superficial muscular tension, the other has a deep bony problem. The meridian diagnosis is identical, but the depth different — and that changes your needle depth entirely. Always ask: "Is it at the surface, in the muscle, or does it feel deep?"
5. Not re-diagnosing after needling
You needle, the patient reports improvement, but there's residual pain — and the residual pain has shifted position. The remaining pain might now be on a different meridian entirely. Re-diagnose: ask the patient to show with one finger where the remaining problem is. This is the feedback loop that makes Balance Method treatments so precise — the same diagnosis skill applied before and after each needle.
Quick Reference: Step 1 Diagnosis
The foundational step: pinpointing the sick meridian by location.
The One-Finger Protocol
| Step | Action |
|---|---|
| 1. | "Show me with one finger exactly where you feel it" |
| 2. | Identify the meridian — which channel runs there? |
| 3. | Note the location — at what level between landmarks? |
| 4. | Assess the depth — skin, muscle, tendon, or bone? |
| 5. | Determine coverage: point, line, or area? |
Meridian Geography at a Glance
| Position | Yin (Medial) | Yang (Lateral) | Arm | Leg |
|---|---|---|---|---|
| Front | Tai Yin | Yang Ming | LU / LI | SP / ST |
| Middle | Jue Yin | Shao Yang | PC / SJ | LIV / GB |
| Back | Shao Yin | Tai Yang | HT / SI | KID / UB |
Diagnosis → Approach
| Patient Shows | → | Your Approach |
|---|---|---|
| One point, one meridian | → | Standard balance (one treating meridian) |
| One line along a meridian | → | Proportional line coverage on treating meridian |
| In-between two meridians | → | Balance both, or find one treating meridian via matrix |
| Two or more separate locations | → | Matrix analysis: find common treating meridian |
| Everywhere / no fixed location | → | Global Balance pattern |
Master the complete matrix of balancing options:
Get the Balance Method NotebookFrequently Asked Questions
Do I really never use tongue or pulse?
Not for acupuncture point selection in this system. If you also prescribe herbs, tongue and pulse remain essential for that purpose. But for needle selection, meridian-based diagnosis gives you everything you need. Many Balance Method practitioners treat four patients in under 40 minutes — all with strong clinical results — because the diagnostic method is fast by design. The only exception might be, for example, when we use Dr. Tan’s 5 Elements for treatment.
What if the pain doesn't clearly fall on one meridian?
That happens often, and it's fine. If the pain sits between two meridians, diagnose it as a two-meridian problem. Use the matrix to find a treating meridian that covers both. If the pain is broad and diffuse, consider whether a Global Balance is more appropriate than a local approach.
What about problems on the head, face, or trunk?
Same principle. The face has Stomach (cheek, jaw), Large Intestine (around the nose and mouth), Urinary Bladder (from inner eye over the head), and Gallbladder (temples, sides). The trunk has meridians along the front (Stomach, Kidney, Ren Mai), sides (Gallbladder, Liver), and back (Urinary Bladder, Du Mai). Identify which meridian runs through the area of complaint — that's your Step 1. Then use an Image projection (puppet show or big image) to find the treating zone.
How quickly can I learn meridian geography?
Most practitioners develop reliable meridian identification within two to three weeks of daily practice. The exercise is simple: trace all six lines on your arm and leg every morning. Front-middle-back, Yin side then Yang side. Within a month it becomes as automatic as reading. The Balance Method Notebook includes visual meridian maps designed for this daily practice.
Next Steps
Step 1 is where every Balance Method treatment begins. Get it right and everything that follows — the system choice (Step 2), the projection and ashi palpation (Step 3) — falls into place. Get it wrong and no amount of system knowledge or projection skill will compensate.
The good news: Step 1 is a skill that develops fast. Within weeks of practicing the one-finger protocol, meridian identification becomes automatic. Within months, you'll diagnose the sick meridian before the patient finishes their sentence — just by watching how they move and where they guard.
Watch needling demonstrations on our needling demo page. For foundational reading in Dr. Tan's own words, explore our book recommendations. And join our practitioner community of 7,000+ members to discuss diagnostic cases and sharpen your meridian identification. New to the terminology? See the Balance Method Glossary for every core term in one place.